Editor's Note, Volume 8 Issue 2


D’Arcy Little, MD, CCFP, FRCPC Medical Director, JCCC and HealthPlexus.NET
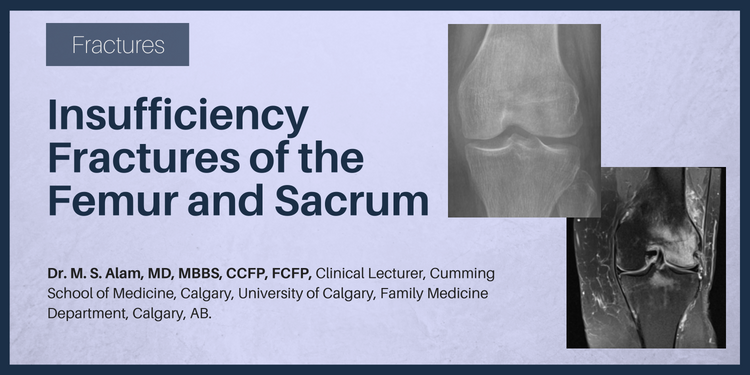
Dr. M.S. Alam, MD, MBBS, CCFP, FCFP
Clinical Lecturer, Cumming School of Medicine, Calgary, University of Calgary, Family Medicine Department, Calgary, AB.
CLINICAL TOOLS
| Abstract: Insufficiency Fractures (I.F) are non-traumatic fractures that occur in abnormal bone (low density bone). Usually occurs in elderly post-menopausal women and is non-traumatic. X-rays are unremarkable and MRI showed extensive bone marrow oedema and subchondral fracture. Ms. Shirley Cooke, a 61 year old with a background of low bone mass, breast cancer, Diabetes Melitis type 2, HTN, splenic artery thrombosis came in with a dull pain on her left knee and occasionally some sharp element, with unremarkable examination on knees. Recently, she was diagnosed with left ankle avulsion fracture of lateral maleolus and is wearing an ankle boot for healing. It is important to make the correct diagnosis in order to avoid complications." |
| Key Words: Insufficiency Fracture (I.F), low bone mass, management. |


| 1. With regard to I.F of femoral Condyle—Although the knee symptoms will always be unilateral, on the side of the meniscal tear, and are more frequent in older woman, the pain of an insufficiency fracture can easily be confused with that of other joint pathologies and therefore be easily missed.2 |
| 2. With regard to I.F of Femoral Neck—This fracture is seen in the elderly osteoporotic patient, often following a trivial event such as a slip without a fall. The resultant boney defect may be a compression fracture, which is inherently stable, or a transverse fracture, more common in older patients and is potentially much more serious. |
| 3. With regard to I.F of Sacrum—The possibility of an insufficiency fracture should be considered in elderly osteoporotic patients, particularly women, following evenly seeming innocuous trauma to the posterior pelvis who exhibit constant buttock pain which may radiate to the thigh or groin and is unaffected by spinal movement. |
| MRI is the gold standard for Dx. I.F. |
| Symptoms and conventional tests may not be helpful, High Index of suspicious is needed. |
| To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app. |
Raphaële Charest-Morin, MD, FRCSC,1 Nicolas Dea, MD, MSc, FRCSC,2
1Department of Orthopaedic Surgery, Centre Hospitalier Universitaire de Québec, Laval University, QC.
2Spine Surgeon, Clinical Associate Professor of Neurosurgical and Orthopedic Spine Program, Vancouver General Hospital, University of British Columbia, BC.
CLINICAL TOOLS
| Abstract: General practitioners are occasionally confronted to unknown lesions of the spine. Recognition of imaging characteristics and anatomic details from the different imaging modalities generally provides sufficient information to generate an appropriate differential diagnosis. Importantly, first line clinicians should recognize worrisome imaging characteristics and initiate timely referral when indicated. On the other hand, lesions expressing benign features should also be identified to avoid anxiety for the patient and overuse of diagnosis imaging studies. In a public health-care system, judicious utilization of imaging is of paramount importance. This article will review an approach to unknown bony lesions of the spine. |
| Key Words: Spinal lesion, tumour, imaging characteristics, primary bone tumours. |
Members of the College of Family Physicians of Canada may claim MAINPRO-M2 Credits for this unaccredited educational program.
www.cfpc.ca/Mainpro_M2
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.

| A solitary spinal lesion warrants a careful investigation. Most of the time, local imaging and systemic staging provide diagnosis. |
| In patients over 40 years old, most tumours are malignant with metastases and multiple myeloma being the most frequent. Benign and incidental lesions such as bony islands and hemangiomas are, however, also frequently encountered in this age group. |
| In patients under 30 years old, tumours of the spine are uncommon and are generally benign with the exception of Ewing Sarcoma and Osteosarcoma. |
| Primary bone tumours of the spine are rare and should be referred to specialized centers. |
| Worrisome features on imaging include aggressive bony destruction, spinal canal invasion, soft tissue mass and multiple level involvement. |
| Pyogenic infections usually start in the disc space, whereas tumours generally spare the intervertebral disc. |
| Most aggressive lesions will initially present with non-specific clinical complaints and as such, a high level of suspicion is warranted. Systemic symptoms are rare with primary bone tumours. |
| Most incidental findings do not require any follow-up or further investigation. |
| To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app. |
Abandoning Treatment Due to Age Alone


When caring for older adults with comorbidities, especially those at the extreme upper limits of life, it may be easy for providers to lessen the intensity of their curiosity and medical investigation. For some older individuals’ chronic conditions, the odds of a positive outcome may seem too distant or the patient’s discomfort—or, in many jurisdictions, the financial burden—may act as a barrier to the pursuit of answers.
- Read more about Abandoning Treatment Due to Age Alone
- Log in or register to post comments