Editor's Note, Volume 9 Issue 2


D’Arcy Little, MD, CCFP, FRCPC Medical Director, JCCC and HealthPlexus.NET
Kedar Padhye, MBBS, DNB (Ortho), 1Reza Ojaghi, MD, 2Fábio Ferri-de-Barros, MD, MSc, FSBOT, FSBOP (Hon.), FRCSC, FCS(ECSA),3
1 Clinical Fellow (Pediatric Spine Surgery)Division of Paediatric Surgery, Section of Orthopaedic Surgery, Alberta Children's Hospital, University of Calgary, Calgary, Alberta.
2Orthopaedic Surgery Resident, Department of Orthopedics, University of Ottawa, Ottawa, Ontario.
3 Department of Orthopedics, Alberta Children's Hospital, Calgary, Alberta.
CLINICAL TOOLS
| Abstract: Adolescent Idiopathic Scoliosis (AIS) is defined as curvature of spine in the coronal plane with a Cobb angle of more than 10°. AIS affects 1-3% of children younger than 16 years of age. Less than 20% of those children will progress to severe deformity requiring interventions. Screening with clinical examination and selective radiographic assessment seems to be a cost-effective approach to filter specialist referrals but current literature is controversial. Evidence supports brace management of AIS for skeletally immature patients with primary scoliosis measuring 25°–40. The risk reduction for progression to the surgical range (deformity greater than 50 degrees) is 56%. Timely diagnosis and evidence-based brace management of AIS seem likely to reduce the surgical burden. The implementation of screening guidelines at the primary care level is a critical step. |
| Key Words: scoliosis; idiopathic; Brace treatment; conservative treatment; screening. |
Members of the College of Family Physicians of Canada may claim MAINPRO-M2 Credits for this unaccredited educational program.
www.cfpc.ca/Mainpro_M2
You can take quizzes without subscribing; however, your results will not be stored. Subscribers will have access to their quiz results for future reference.


| Bracing is an effective but time sensitive intervention for managing AIS in skeletally immature patients with primary scoliosis measuring 25 to 40 degrees. |
| Clinical screening is required to identify AIS patients who eligible for bracing. |
| Improving access to bracing for eligible patients requires a collaborative approach involving primary care physicians and specialists. |
| 1. A systematic collaborative approach involving primary care physicians for screening patients and referring to tertiary care ensures timely assessment and management for eligible patients. |
| 2. Evidence supports brace management of AIS for skeletally immature patients with primary scoliosisl measuring 25°–40°, with the goal of preventing deformity progression to the surgical threshold. |
| 3. A full time (18-23h/day) rigid brace treatment may mitigate the surgical burden of AIS by approximately 30%. |
| To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app. |
Dr. Robert Caratun, BSc, MSc,1 Dr. Aly Abdulla, MD, CCFP, FCFP, DipSportMed CASEM, CTH, CCPE, McPL,2
1is a graduating medical student from The University of Ottawa going into Family Medicine residency at The University of Calgary in June 2019. He has a background in coaching and creating custom mental skills programs for athletes.
2 is a family doctor with specialties in sports medicine, palliative care, and cosmetic medicine. He can be found on Twitter, LinkedIn and https://ihopeyoufindthishumerusblog.wordpress.com/
CLINICAL TOOLS
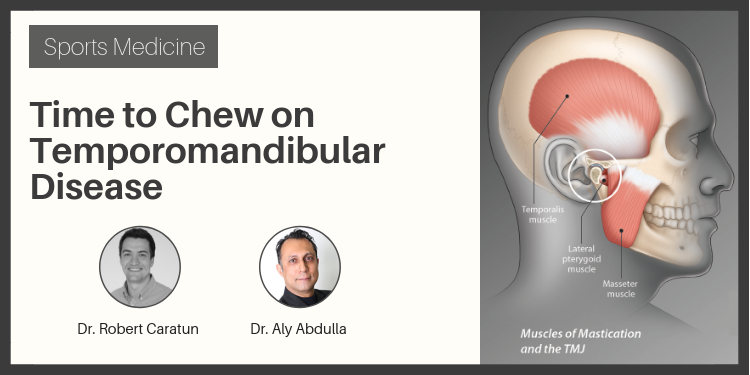
| Abstract: Temporomandibular disorders (TMD) are one of the most common non tooth-related chronic orofacial pain conditions that involve the muscles of mastication and/or the temporomandibular joint (TMJ) and associated structures. This article reviews the etiology, diagnosis, and treatment of this chronic pain condition. |
| Key Words: chronic pain, temporomandibular disorders (TMD), temporomandibular joint (TMJ). |





| 1. The etiology of TMD is multifactorial in nature |
| 2. TMD is a clinical diagnosis. Clinicians should perform a complete history and physical with special focus on a dental and psychiatric history. |
| 3. Imaging can be considered if history and physical are insufficient for diagnosis. Diagnostic injections can also be used to further guide clinicians. |
| 4. For TMD treatment, supportive patient education should be prioritized (jaw rest, soft diet, passive stretching) in addition to conservative treatment measures (e.g. NSAIDs). |
| The most common presenting symptoms of TMD are facial pain, ear discomfort, headache and jaw discomfort/dysfunction. |
| Symptoms of TMD are typically associated with jaw movement and pain in the temple, masseter, or preauricular region. If there is no pain with jaw movement, consider an alternate diagnosis. |
| A large volume of patients report abnormal jaw sounds with no jaw pain or dysfunction. Do not treat adventitious jaw sounds; only pain or discomfort in TMD |
| Patent supportive measures and conservative treatment result in significant pain reduction for the majority of patients and should be the main focus of TMD treatment. |
| To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app. |
Yoni Freedhoff, MD,
Family doc, Associate Professor at the University of Ottawa, Author of The Diet Fix, and founder of Ottawa's non-surgical Bariatric Medical Institute—a multi-disciplinary, ethical, evidence-based nutrition and weight management centre. Nowadays I'm more likely to stop drugs than start them. You can also find me on Twitter and Facebook.
CLINICAL TOOLS
| Abstract: The reason why weights rise in the industrialized world remains unclear, but most agree that diet plays a crucial role. The endless list of fad diets from paleo to keto to low-carb has led to public mistrust and confusion. The results of a new study titled "Ultra-processed diets cause excess calorie intake and weight gain: A one-month inpatient randomized controlled trial of ad libitum food intake" strongly suggests that regardless of diet, ultra-processed foods should be avoided. |
| Key Words: diet, nutrition, ultra-processed foods, calorie intake, weight gain. |


| Helping patients understand the importance of limiting the consumption of ultra-processed foods may be the first step to a healthier lifestyle. |
| Suggest planning meals ahead of time and eating healthy fats (olive oils, avocado, nuts), grains, enough protein (fish, beans, nuts) and fresh fruit and vegetables. |
| Discuss how ultra-processed foods may well be a contributor to both weight and other diet related diseases. |
| Reducing or eliminating consumption of ultra-processed foods may be an effective strategy for obesity prevention and treatment, but doing so requires privilege, time, skill, and expense. |
| To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app. |