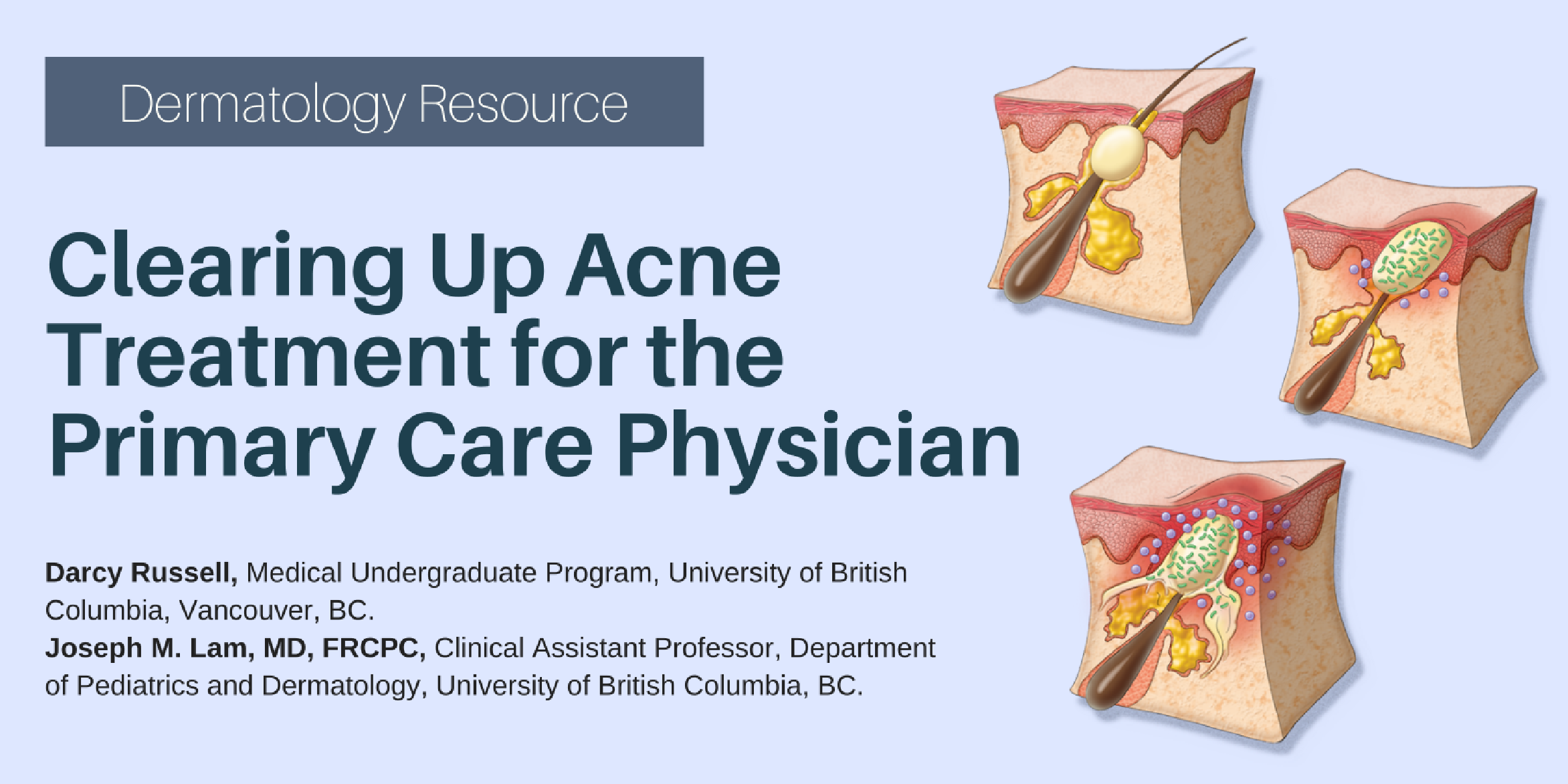
Pathogenesis of Acne Vulgaris
Year
2011
Number
3
Image Number
1
Related Article
Image Galleries
- Read more about Pathogenesis of Acne Vulgaris
- Log in or register to post comments