About Psoriasis
WHAT IS PSORIASIS?
Psoriasis is a common but chronic skin condition that causes
inflammation and scaling (red elevated patches and flaking silvery
scales). The patches can be itchy or sore, causing discomfort and pain.
Psoriasis causes skin cells to rise to the surface and shed at a very
rapid rate. On average, people with psoriasis shed their skin cells
every 3 to 4 days, while people without the condition have a turnover
rate of about every 30 days.1,2,3,4
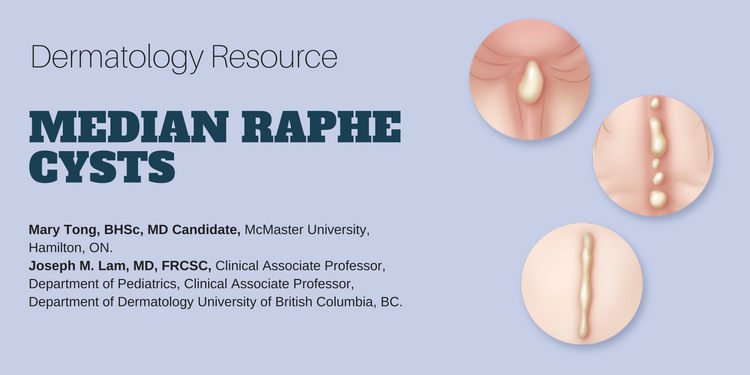
Mary Tong, BHSc, MD Candidate,1 Joseph M. Lam, MD, FRCSC,2
1McMaster University, Hamilton, ON.
2Clinical Associate Professor, Department of Pediatrics, Clinical Associate Professor, Department of Dermatology University of British Columbia, BC.
CLINICAL TOOLS
Abstract: Median raphe cysts are rare congenital lesions caused by a defect in embryological development of the male genitalia. They can present as solitary or multiple papules along the median raphe from urethral meatus to the anus. Although they are asymptomatic during childhood, they can cause problems later on as they increase in size. Surgical excision of the lesion is not necessary unless the patient becomes symptomatic.  |
| Key Words: median raphe cysts, congenital lesions, treatment, management. |



| Median raphe cysts are benign cysts that can be present at birth, or acquired due to trauma or infection in the genitalia area. |
| Histologically, the cysts can have pseudo stratified columnar, squamous cell, or glandular epithelium, or a mixture of these cells. |
| Although these cysts are asymptomatic during childhood, they should be monitored overtime because they may cause problems as they increase in size with time. |
| Because these are benign malformations, median raphe cysts do not require excision unless they cause problems such as pain, problems with urination or sexual activity, or for cosmetic reasons. |
| Median raphe cysts are benign lesions that may be caused be a defect in the embryological development of the male genitalia. |
| The differential diagnoses of median raphe cyst include glomus tumor, dermoid cyst, pilonidal cyst, epidermal inclusion cyst, urethral diverticulum, and steatocystoma. |
| Treatment for asymptomatic median raphe cyst is not necessary but surgical excision can be considered if the cyst is causing problems or for cosmetic reasons. |
| To have access to full article that these tools were developed for, please subscribe. The cost to subscribe is $80 USD per year and you will gain full access to all the premium content on www.healthplexus.net, an educational portal, that hosts 1000s of clinical reviews, case studies, educational visual aids and more as well as within the mobile app. |
About Rosacea
WHAT IS ROSACEA?
Rosacea is a common, chronic skin condition that causes redness of the face. It often presents as a mild redness or blushing that, over time, lasts for longer durations and becomes more pronounced. Rosacea can also produce enlarged, visible blood vessels and small red bumps on the facial skin. Before diagnosis, it can be mistaken for acne, an allergic reaction, or other skin conditions.1,2,3
Frequently Asked Questions about Psoriasis
WHAT IS PSORIASIS?
Psoriasis is a common but chronic skin condition that causes
inflammation and scaling (red elevated patches and flaking silvery
scales). The patches can be itchy or sore, causing discomfort and pain.
Psoriasis causes skin cells to rise to the surface and shed at a very
rapid rate. On average, people with psoriasis shed their skin cells
every 3 to 4 days, while people without the condition have a turnover
rate of about every 30 days.1,2,3,4
Living with Psoriasis
CARING FOR YOUR SKIN
Frequently Asked Questions about Rosacea
WHAT IS ROSACEA?
 |
Rosacea is a chronic skin condition that mainly affects the skin on the face (cheeks, nose, chin, and forehead).1 Living with RosaceaCARING FOR YOUR SKIN
|












